A ventricular septal defect (VSD) is an abnormal openning between the right ventricle and the left ventricle. VSD’s occur both as isolated lesions and in combination with other lesions, such as coarctation of the aorta. There are several types of VSD, categorized by their anatomic location
- Membranous (or perimembranous) VSD is located in the membranous septum, in proximity to the tricuspid and aortic valves. About 80% of VSD’s are of this, the most common, type.
- Subarterial or supracristal VSD’s are located close to the aortic valve. About 10% of VSD’s are this type.
- Muscular VSD’s are located in any area of the ventricular septum
- Atrioventricular canal type VSD’s are located under the tricuspid valve
Physiology
The abnormal connection between the ventricles in VSD’s allows blood to flow across the defect from one ventricle to the other. The amount and direction of flow is controlled by a) the size of the VSD, more blood flowing across large VSD’s and b) the resistance of the downstream vascular bed, that is, the pulmonary vascular resistance (PVR) and the systemic vascular resistance (SVR). If the PVR is low and the SVR is high (the usual circumstance in childhood) flow will be from the left ventricle to the right ventricle (left to right).
Pathology
The abnormal flow across the VSD may have several direct and indirect deleterious effects. The increased flow from the left side of the heart to the right side of the heart then flows through the pulmonary bed. This increased flow is then recirculated through the right heart and can lead to right heart enlargement. In addition, the increase flow in the pulmonary vascular system can damage the pulmonary circulation, leading to pulmonary vascular obstructive disease, an irreversible condition.
In addition to adverse effects from increased flow, turbulence created by flow across the VSD may lead to damage to the aortic valve. This damage is not necessarily related to the amount of flow across the VSD and in fact the involvement of the aortic valve may decrease flow across the VSD. Damage to the aortic valve is not reversible and may be severe.
Surgical Indications and Approach
Some VSD’s may close spontaneously. Small muscular and small perimembranous VSD’s may close spontaneously in the first few years of life). AVSD that is being partially closed aortic valve tissue is a very dangerous situation and frequently requires surgical intervention.
Symptomatic patients are operated on when the lesion is discovered. Symptoms may include rapid breathing, shortness of breath, poor weight gain or poor exercise tolerance. In addition, any patient with significant involvement of the aortic valve (aortic insufficiency, or a leaking aortic valve) should be operated on expeditiously.
Asymptomatic patients are operated on depending upon the amount of blood flow across across the VSD (shunt). In general, patients with more than a 50% increase in blood flow through the lungs require repair.
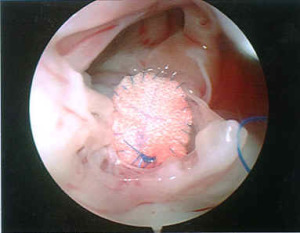
Ventricular septal defects are typically closed using the heart lung machine and by placing a patch over the defect. The patch may be a piece of fabric (Dacron) or the patient’s own tissue (pericardium) and it is secured with fine sutures.