Anatomy
The ductus arteriosus is a normal structure that is open (patent) during normal fetal development in the womb. It connects the pulmonary artery with the aorta. In the womb, it allows blood to flow around the lungs rather than going through them. In most full-term infant the ductus closes spontaneously in the first hours to weeks following birth. It remains open more frequently in premature infants with low birth weight. In addition, the patent ductus arteriosus not uncommonly associated with other congential heart lesions, such as atrial septal defect, ventricular septal defect and single ventricles.
Physiology
The patent ductus arteriousus is an unnatural connection when it remains open after birth. It connects the pulmonary (blue blood) circulation to the systemic (red blood) circulation. Blood flows across the ductus depending on the relative resistance on the pulmonary circulation (pulmonary vascular resistance, PVR) and systemic circulation (systemic vascular resistance, SVR). In the usual circumstance the SVR is high and the PVR is low and therefore, oxygenated blood flows from the systemic circulation into the pulmonary circulation. This results in increased pulmonary blood flow.
Pathology
A patent ductus arteriousus may have several pathological consequences. The increased pulmonary blood may lead to heart failure, and pulmonary vascular obstructive disease. In addition, the abnormal flow patterns across the ductus creates an increased risk of bacterial endocarditis (infection) of the heart and ductus itself. The infection, or rupture of the ductus, may be fatal.
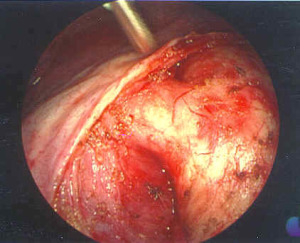
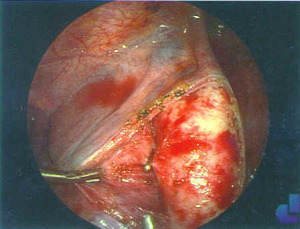
Surgical Indications and Approach
A patent ductus in an infant older than three months or so, or a symptomatic ductus in a premature infant or a neonate, is an indication for closure. Closure may be accomplished electively, usually before 2 or 3 years of age.
There are three usual approaches to closure of the patent ductus arteriousus: open closure via a thoracotomy (a chest incision covering about half the ribcage on the left side): closure using a tiny video camera and three or four small incisions (Video Assisted mini Thoracotomy, VATS) or, in some cases, closure via a metal device delivered by trans-arterial catheter. In all cases, the aim of the procedure is to completely and permanently close the ductus