Coarctation of the aorta occurs either alone (simple coarctation) or in association with other lesions, most commonly with ventricular septal defect. Coarctation of the aorta most commonly occurs just past the origin of the left subclavian artery, the artery that carries blood to the left arm. The narrowing is in the area that that the ductus arteriousus inserts into the aorta. There is a wide variation in associated problems. This discussion will refer to simple, isolated, coarctation of the aorta
Physiology
The narrowing in the aorta obstructs blood flow from the heart to the lower body. In the most severe forms of coarctation, blood flow to the lower body may depend on a patent ductus arteriousus.
Pathology
The obstruction to blood flow may result in organ damage in the lower part of the body (kidney problems, problems with the bowel), problems with the heart (heart failure) and high blood pressure above the coarctation.
Coarctation of the aorta may present several different ways. In infants, coarctation may present with diminished femoral pulses, difficulty feeding and heart failure. In older children, coarctation of the aorta may be discovered in a routine physical exam or during an evaluation for high blood pressure.
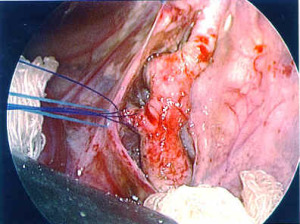
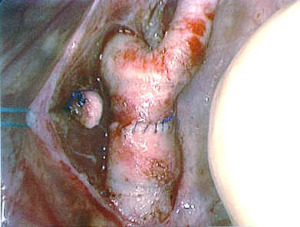
Surgical Indications and Approach
In general, significant coarctation of the aorta in infants is repaired soon after discovery. Significant coarctation in children should be repaired expeditiously. There have been many operation performed for coarctation of the aorta. The goal of every operation for coarctation of the aorta is complete repair and long-term success. Literature rates for re-coarctation in neonates range from 10 to 20%.